Discussion
The concept of torque has been around for decades. Its foundation to create a circular motion that turns C2 directly is incorrect. From its inception it has never been revisited, revamped, or rethought. Each new generation has continued to teach information without re-discussing its current truth and validity. This article will revisit the concept of torque, provide a new, fresh look that also discusses when torque is applicable and its necessity in certain misalignment types.
The Newtonian Law article (8/2010) discussed the concept that the primary misalignment occurs at the lower angle and the C0/C1/C2, despite its neurological significance as the body’s upper compensation mechanism. Some bullet points that will help in the torque discussion are:
- C2 – Pelvis moves as a closed kinetic chain
- Large masses dictate the movement of small masses at equal velocity
- The pelvis is the largest lever in the human frame
This information, from a biomechanics foundation, questions the model that C2 is the measurable point to detail torque. This is because C2 is the smallest mass of the lower angle (consisting of C2 through Pelvis). So, how can it be the great force to move everything below it? It can’t! This is why the pelvis is the predominant factor. It dictates the sagittal-torsional breakdown of the lower angle and minimizes C2 as only a compensator. The mass of these two bones is the first error that makes the case for the pelvis.
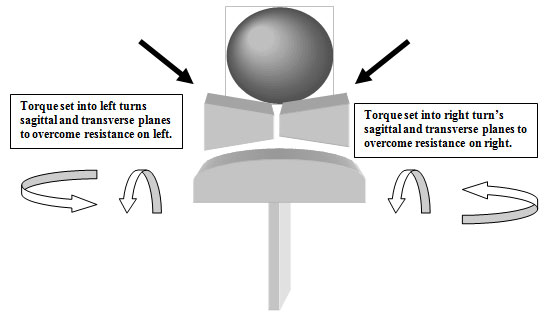
The second point that is raised to question our present understanding is the thought that torque moves the frontal plane. This is not based on the motion of the adjuster and the cupping structure of C1 and C2. C1 and C2 are connected in a concave-convex relationship. The base of support (C2) is shaped like a sphere and as the circular vector of torque hits the sphere it has both sagittal and transverse plane action. This action changes based on the height-to-rotation relationship and is detailed below.
Summary
- The pelvis is the largest mass of the lower angle and is the predominant factor to determine torque.
- The circular force of torque acts on the lower angle and skull in the sagittal and transverse planes specifically.
For the Physicists out there!
As mentioned above, torque acts on two levels. It is a coupled motion of the sagittal-torsional (circular) and transverse (linear) planes. Torque is a circular component and can be defined as a particle in a rotating body. It has a particular angular speed about an axis of rotation.
The atlas is basically pinned between two upper spheres (condyles) and a lower sphere, C2. The skull has its respective right and left spheres – each with its own axis of rotation around the atlas. Furthermore, the atlas will turn in a circular coupled motion around its own axis of rotation called the odontoid. Although they can move in opposite circular pathways, they are dependant on each other due to their action as one closed kinetic chain. In a rigid body such as the skull, spine, and pelvis, the direction of forward/backward spin, or rotational inertia acting on the spin in counter-clockwise or clockwise direction, is dependant on the side of the C2 surface on which it is applied. Simply, because the surface of C2 is elliptical or rounded, the placement of the force at different points of C2 will affect the structures above and below in very different ways. Torque in the correction creates a coupled motion in the sagittal-torsional and transverse planes.
To visualize this further in terms of spinal mechanics:
A sphere (C2 or the occipital condyles) can be divided into four quadrants (right, left, anterior, and posterior) to further explain the direction of a force. Each quadrant has infinitesimal vector projections as a function of direction and an exact 180-degree mirror image of directional complement – right and left, and anterior and posterior. This 180-degree vector will allow a directional change of the torque without altering the leverage necessary for a proportional three-dimensional correction. This concept of setting the skull against the appropriate C2 and C0 surfaces is the key to correcting the linear (transverse) as well as correcting the torsional (sagittal) component of the misalignment.
The Hand
At present, we are unable to measure what part of the misalignment is sagittal-torsional or transverse. The action of torque through the feel of the adjuster as the resistance breaks is at present the only deciphering mechanism. The hand correction with its wrist lever is the only way to correct pathways. The UC adjusting machines without a circular path motion and the ability to lever against the resistant point are unable to overcome this resistant pathway. This is why the wrist lever in the correction is the overcoming resistance function in all spinal corrections.
How to Measure Torque
Posture measurement of the pelvis is the key indicator for which torque is required. This is determined by measuring the pelvic rotation (anterior/posterior) on the weighted side. This is then used in the protocol for skull and pelvic placement to access the circular pathway. The Anatometer and its calipers, laser light belts, and portable calipers are subjective and significantly inaccurate. Our lasers measure the pelvic rotation by establishing a fixed point behind the Anatometer and measuring a distance to each similar PSIS (see laser lights on patient).

General Rules:
Inferior torque: For a posterior pelvis
Superior torque: For an anterior pelvis
Torque is always measured on the weighted side.
Torque has different actions based on the relationship between the height and rotation. This is called the 45-Degree Rule.
The 45-Degree Rule
Different Actions of Torque: Understanding the 45-Degree Concept
Torque can have two actions, namely transverse and sagittal. The relationship of the height-to-rotation dictates the predominance of either rotational movement or front-to-back movement. This is extremely important when analyzing the necessary headpiece placement for an out-of-pattern misalignment (OPM).
The Relationship:
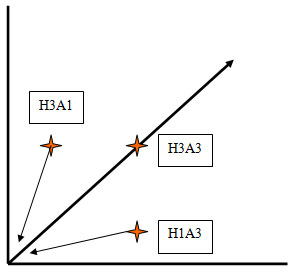
Height, rotation, and the notch transverse have a relationship that creates a horizontal resultant. The horizontal resultant exists either above the 45-Degree, below the 45-Degree, or on the 45-Degree.
For example:
High 1” Anterior 1”, High 2” Anterior 2”, etc.
Creates a horizontal resultant (HR) that is exactly a 45-degree angle. When torque is introduced at this vector, or at any vector on the 45-degree, it has equal action on the transverse and sagittal planes.
High 3” Anterior 1”
Creates an HR that is above a 45-degree angle. When torque is introduced it has more of a sagittal action than a transverse action. As the height to rotation relationship increases above the 45-degree mark, the more sagittal to transverse action occurs.
High 1” Anterior 3”
Creates an HR that is below a 45-degree angle. When torque is introduced it has more of a transverse action than a sagittal action. As the height to rotation relationship increases below the 45-degree mark, the more transverse to sagittal action occurs.
Application of Torque:
The application of torque will be dependent on Anatometer readings. The correct torque is viewed on the Anatometer as the sagittal torsional or transverse component of the weighted pelvis. If the weighted side measures posterior with the lasers, then the torque is inferior. If the weighted side measures anterior with the lasers, then the torque is superior.
Torque
Torque has a dual action on the spine. It has a transverse and sagittal action. The height-to-rotation relationship dictates which plane receives more action.
It is only indicated when:
- There is a counter-rotation between C1 and the Pelvis
- Upper angle and the lower angle are non-linear if lower angle was filmed correctly without shoulder twist (see Nasium x-ray placement)
Note:
- The torque you use is accomplished by closing the quadrant desired, i.e., Posture-Right 16 lbs P10 mm close RP and use inferior or CCW torque
- Some misalignments need both inferior AND superior torque. Inferior torque on one side and superior torque the other. That does not mean turning the patient over, but adjusting the headpiece to close the appropriate quadrant.
When is torque applicable?
Torsional pathways, like other pathways, can always be found. The question is their importance and predominance to the correction and spinal stability. This is only known when checked tactilely by the practitioner. This skill separates us at QSM3 and our ability to complete the correction among other hand and machine adjusters. The inability to feel limits your ability to “flatten all pathways” and know if other pathways exists.
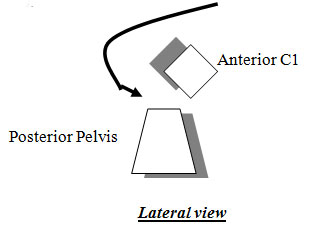
Torque is necessary in certain misalignments – namely the counter-rotated. The counter-rotated configuration is where the C1 and pelvis are opposing or in opposite transverse planes. One is anterior and the other is posterior. When this configuration is presented, torque is a necessary function to access and clear the opposing directional planes. It allows the force to enter at the C1 and reverse the transverse and sagittal-torsional vector similar to a boomerang.
An anterior vector with a posterior pelvis would dictate inferior torque (counter-clockwise-CW) to travel down the pathway P to A and correct the posterior pelvis.
Summary
The torque is a function of the pelvis and affects the sagittal-torsional and transverse planes of the primary pathways of the lower angle (C2-pelvis). The skull and C1 are secondary compensators. Torque is also a circular motion that only the hand can access through touch and motion.
Finally, the posterior pelvis on the weighted side uses CCW or inferior torque, and the anterior pelvis on the weighted side uses CW or superior torque. Its action is proportional to the height and rotation relationship.
Setting Torque
- Measure the weighted side
- Measure the posterior or anterior pelvis on the weighted side
- Skull placement – close the C0/C1/C2 articulation of the weighted side
- Lift the chin to close the posterior quadrant for inferior torque
- Tuck the chin to close the anterior quadrant for superior torque
- Feel the pathway
- No matter what side you are implmenting torque (right laterality/right side weight – torque on right laterality/left side weight – torque etc.) inferior torque is always CCW, superior torque is always CW
The discussion of torque is best accomplished through a classroom and lab format. I hope this discussion helps with your counter-rotated C1 and Pelvic misalignments. Awareness is the first step to resolution.
Finally, torque is a function of the wrist lever and not the triceps. It is the primary mover to reverse the direction of the counter rotated C1 to Pelvis. The tactile development of the practitioner is the highest level. I have seen films clear and pathways still exist.
To develop all these skills and comprehend the path to 3D pathways, there is only one road available…. QSM3
On Purpose and In Progress,
Russell Friedman, DC