A QSM³ Protocol Idea
by Andrew Smyth DC
Dr. Russell Friedman is unbelievable at visualizing the misalignment. I am not quite as visual, and just finally getting around to fitting my anatometer with laser measurers, I had to find a different way to apply the QSM³ concepts. By gently touching and pushing on patient’s body in the standing position, information can be gleaned to direct the pathways to be adjusted. Using this methodology has helped me understand and feel primary pathways, multiple pathways, ripples, torsion patterns, and more deeply understand the nature of people’s misalignment and how to correct them in a more efficient and complete manner.
It can be used in concert with the anatometer, and it can be especially helpful if you do not have laser measures fitted yet. I have recently moved my anatometer in between 2 rooms and, on occasion, I have used this instead of checking on the anatometer after each and every correction. I hope you find this analysis and information helpful in understanding misalignments and making even better corrections and releases, it has definitely done so for me.
The body’s ideal state is aligned, balanced, up and open…but that is not where most people are. Most people are misaligned. Something has to hold the body in this twisted state after injuries to the muscle, tendons, and ligaments that lock it in place.
Most people have multiple layers or levels of misalignment. By combining Dr. Friedman’s quadrant concepts with anatomy trains, and gentle palplation, the pathways of misalignment can be located, released, and confirmed.
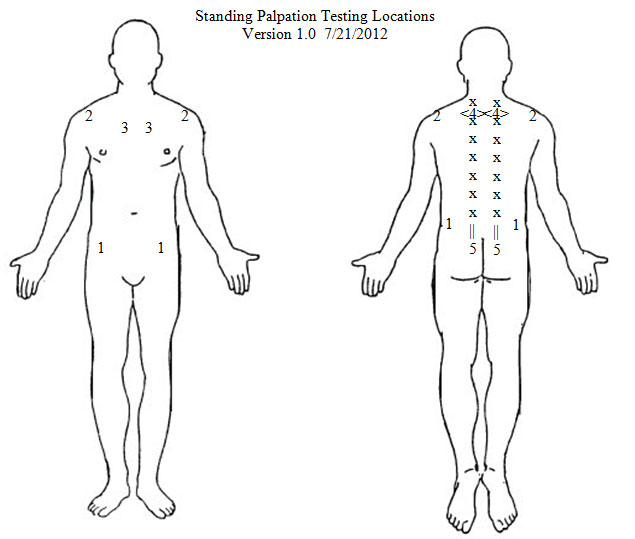
I call the assessment standing palpation, since the patient is standing
The easiest one to feel is in the pelvis.
Lightly touch and push the ASIS posterior and PSIS anterior on each side and feel for a locking of the body. If there is no resistance, the body will rotate and move with touch easily, but if there is resistance in the quadrant, then the body locks and the whole body moves forward. There are levels to it, and the tightest quadrant is the layers and quadrant to address. This is typically on the weighted leg side, but not always.
If there is a weighted leg measurement of R10, there can 1-4 quadrants of resistive tension in the pelvis, the more quadrants, the more complex the misalignment.
The biggest block or tension pattern is the primary or one to address.
I usually coordinate the tension pattern with the weighted leg and/or low shoulder.
Again, this does not always hold true, but it does in ¾ of cases so far.
This can be very helpful if you don’t have an
If we return to the example of R10 and feel a lock or tension at the anterior aspect, then directing the force to A-P on the right side can and will release this tension as long as it is the primary (read strongest) tension pattern.
After the correction, and a repalpation can confirm or deny that the goal was accomplished. This rule will follow the posture pattern, so if the right pelvis is obviously rotated anterior on the right and posterior on the left, then either the right anterior or left posterior pattern will be primary and it is almost always on the weighted side (think what it pulling the person off center).
Sadly for me, just releasing all 4 quadrants of the pelvis, did not guarantee a complete correction or long term stability. I started finding multiple pathways, ripples and torsion.
Currently I start at the pelvis, but I also check 5 other areas for resistive tension. Each give you a piece, and I am still sorting out their order of importance.
- Pelvis at ASIS and PSIS
- Front and back of the shoulder.
- 1-2 inches lateral of mid sternum
- Just medial to scapula just above scapular angle
- Entire paraspinal musculature, feeling for ripples and torsion.
I currently address the most prominent layer first and work people through till, the weight imlance drop below 3 lbs, I make a significant change, or I run out of time.
Using this protocol, I find people do progress through layers and each layer of release often causes the patient to have another experience of opening, ease, lightness and loosening (which I call getting off their nerves).
I do not have enough data, to comment on strength of stability or improved holding using this methodology. In fact, I am curious about creating a resilient correction myself. I am always finding more layers I can release on a majority of patients.Version 1.0 7/21/2012