Introduction
QSM3 is a specific system to direct the calculated vector down the correct resistant pathways and to understand what direction the resistant must be overcome (leverage points). These two factors are fundamentals that, when mastered, will elevate each practitioner significantly. Basically, the better your understanding of what you have to fix, the better your ability to fix it.
There are three aspects to correcting the spinal misalignment consistently. The vector, analogous to a key, is calculated from the X-ray. It establishes the relation between the skull, C1, and the lower angle through pelvis. The posture analysis is like the door lock. It details the headpiece placement, the skull placement, and the patient placement. This is the step that stacks or creates the pathway to ACCESS the misalignment pathways so they can be found and overcome. Without the knowledge or the ability to set these pathways, a complete correction is random at best. The final step is the ability to break resistance. This is analogous to turning the key. Resistance must be overcome in specific tissue pull directions by the wrist lever (leverage points). Leverage points are the direction to tissue pull.
So X-Ray makes the key, the posture details the access to the lock, and the leverage points open the door.
The knowledge of the direction of the wrist lever is determined by the integration of the data of the posture and the x-ray cervical series. It is the dynamic that allows a vector to be re-directed to overcome resistance anywhere in the spine. Most upper cervical procedures change the vector in an attempt to produce the same goal. However, it is a random system that is not scientifically reproducible, consistent, or teachable.
Examples
To demonstrate this concept, let’s say:
C1 is rotated posterior on the right and the pelvis is rotated posterior on the left. The vector in this example would increase the lower angle rotation (i.e., the pelvic twist would increase). You have an out of pattern type; one where laterality is right but the fixed point is left and posture weight 25 lbs. on the left. The correction vector will only move the person more off vertical. The present system is to lower the vector after aligning your x-ray machine, perfect patient x-ray set-up, using a laser cut template to measure ¼ degrees… and then to just randomly change the vector seems @*$%)&@#$!!! [Is this edit correct?]
It is the QSM3 system that details this beautifully with placement and leverage points. It is the most complete progressive Upper Cervical procedure.
Making a point just for fun…everything changes
Leg: L1/2”
Posture: Left 12 lbs. Posterior 1mm FP R.6,
Listing: RH4P2
Questions
- First visualize the misalignment from skull to pelvis
- What is the headpiece placement?
- What is the predominant issue?
- Where is the contact point ý one or two??
Answers
- Do you see the vector will increase the pelvic rotation and drive the patient more left?
- The placement is to drop the head and lift the chin. This will access the LP quadrant or pathway to redirect the vector to go left to right and p to A on the left side
- The 12 lbs on the left is the primary
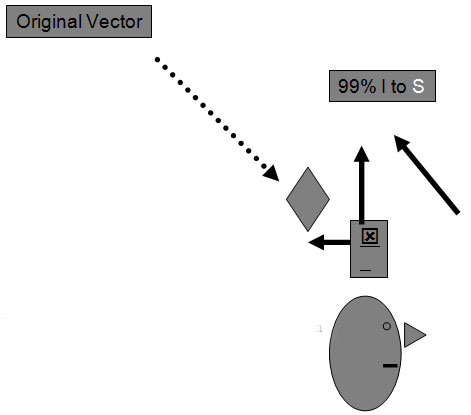
- Below the contact to lever upward to redirect the force I to S to correct the left frontal plane pathway. Also, you need an anterior contact to redirect the force P to A on the left
This concept like most new ones seems overwhelming. Don’t quit this concept; it will be one that elevates your game more than all your understanding about biomechanics in total! With some practice and our seminar, you will realize the ease of this concept and the depth at which it changes your abilities.
Next month we will continue this leverage and the wrist lever.
Russell 5-2011