Gravity vs. tensegrity is a lifetime battle. When we are young and filled with energy, our ability to overcome the compressive forces of gravity, even in a misaligned position, is possible. But as we age and our energetic abilities diminish, gravity always wins. We see the long-term effects of gravity and misalignment in our kyphotic elderly. The breakdown of the spine is not limited to the chiropractic model of our nervous system. As the spine breaks down in all three planes, it is subject to compressive and tensional forces as it struggles to maintain a nonlinear upright position. In chiropractic we see this as short leg, x-ray misalignment, heat differentials, atlas tipping, pelvic distortion, and changes in cervical curves, etc. The truths of all procedures are validated within this broader 3D scope.
Our present misalignment protocol is to compare bone to bone – that is the definition of the mechanistic model. This limits our ability to see the complete breakdown of the misalignment as a ‘system’. With the advent of the Anatometer, Gregory was the first to talk about pathways and the connection to our pelvis. In order to understand how to correct the complete human frame, it is clear that we must first measure the pathway between the breakdown and the corrective reference point (known in vector-based upper cervical work as orthogonal).
Our predecessors’ model of breakdown includes the skull, the atlas, and the neck, which excludes the largest mass of the body – the shoulder girdle to the pelvis. This is the present focus of QSM3.
From knowledge of the breakdown comes the ability to know the reverse pathway to correction, orthogonal, and ultimately tensegrity.
Our focus has turned to this corrective approach based on our knowledge of the pathway of the breakdown. From the compressive forces of gravity the breakdown pathway of the misaligned spine is in a ‘downward spiral’. This is a key conceptual model. In a manner very similar to a screw, the body breaks down in a spiral. This relieves the pressure as it collapses toward the solid floor beneath. If you think about this for a moment, the downward plane of 6 (up, down, right, left, back, and front), you will realize that the downward plane is the only one that has a solid surface against us. This means the break down from gravity and its compressive effect must be integrated or absorbed into the human frame as it collapses. This is the spiral we see in the rotation of the pelvis. Thought of this way, we can understand that to truly correct the misalignment, we must reverse the path of breakdown. The reverse towards tensegral orthogonality can then be successful through an upward un-spiraling.
The indicator of the downward collapsing spiral of tensegrity is not only measurable but must be primarily removed before any other plane can be corrected. The twist (transverse plane) of the pelvis is a direct measurement of collapse. The bigger the collapse – the larger the pelvic twist. The first corrective care process in the QSM3 protocol is therefore to remove all twist in the pelvis prior to addressing any other plane of breakdown.
If the compression still exists, the correction cannot hold optimally.
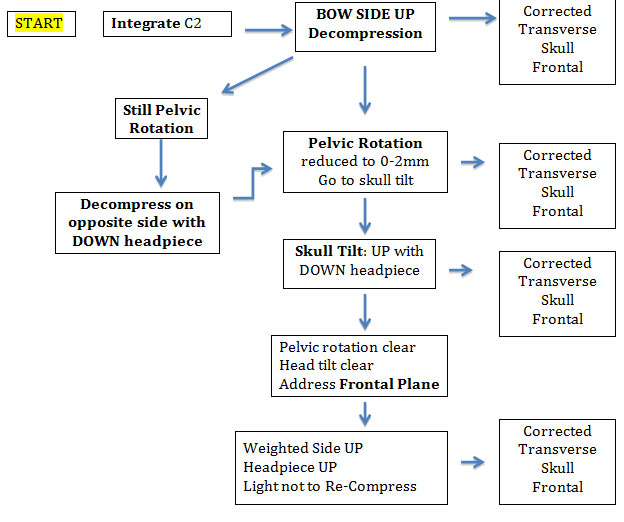
Correcting the compression starts with the concavity of the BOX UP. The mechanical weight of the skull in a downward headpiece position is used to create an opening of the compressed BOX. When the post-adjustment digital scales show the pelvis balanced in the transverse plane, then decompression is complete. However, if not, the patient MUST be flipped and decompressed on the contra-side. It is clear that the correction process cannot move forward until decompression is completed.
I have seen multiple cases that require this double decompression and my logic of “why” points to an S curve and our Accessing Pathways concept. Two opposing concavity curves require two sides of decompression. I imagine most curves are S curves but when one decompression side clears both, the second one was not stuck and compensatory. When one side does not clear both, it points to two pathways that must be accessed to clear the compression.
As the protocol grows, we will be able to help more patients. At present, I use the algorithm below.